

Tasks and Tickboxes: a broken care system.
Last year was a roller coaster of a year and it made me reflect on how i can be more intentional with what i consume all round and not just food but also digitally. I focused alot on my health, getting relevant checks and follow- ups as well as my mental health. As someone with a long term health condition and getting on in age, i needed to stay on top of things. My cholesterol levels have been high for awhile but not of much concern as my good cholesterol was higher than the bad, so that bought me sometime in terms of cardiovascular disease risk.
This has been the healthiest eating combined with fasting that i have done in a long while. I was also conscious of how perimenopause was playing havoc with my body and hormones and no matter what i did, i could not shake the belly fat and the creeping weight gain. Anyhow, i ploughed on and even got joking with the family about how my Doctor will tell me my cholesterol levels have gone up despite all my healthy habits! Come the new year, i had my half yearly check and bloods and was very confident that even though my weight was still on the high side, my cholesterol levels would at best decrease or at worst stay the same.
I get the call from my consultant and everything is fine except the bloody cholesterol and the levels mean that a recommendation will be made to my GP to consider starting me on statins after having a discussion. I am not a fan of statins or regular medication especially if other options are available, so while i waited for an appointment from my GP to discuss my options,as had been suggested by my consultant, i drew up a list of questions and concerns i had.
A week and a half later i get a call from the GP surgery and it is the pharmacist calling to discuss my high cholesterol levels, if the hospital had given me any statins and if not then which ones she could prescribe. she then asked a series of questions about my activity levels and diet with the offer to send me a link to healthy eating. She checked which pharmacy i collect my medication from, informed me that i would experience some side effects when i started the prescribed statins but not to worry. I was then to have repeat blood tests in 6-8 weeks and did i have any questions? To say i was stunned into silence would be an understatement.
I was mad and disappointed, not at her but at the system that is broken and has been reduced to a task based and tickbox service where the whole sum of the person and their circumstances and views are not taken into account or made space for, when their care is being decided. I know the days of having a meaningful face to face conversation with your GP who had all your records at hand and had known you for years are over, but i had at least expected to have a face to face appointment to discuss this life changing event and explore other options available. That i would be given the chance to make an informed decision instead of the decision being made for me.
So for now i have a prescription waiting for me that i am not keen on picking up any time soon. Meanwhile i am intent on pursuing those alternative methods like exercise and diet and see what results i get when i next have my blood test. What is it they say? You are more likely to look after your health if you are involved in the decisions about it and are invested in it. Please talk to and with patients and not at them. When patients feel they have a say in their health and care they are more likely to be receptive to suggestions made and not balk at them.

Self-Swabbing Vs In-Person Smear Test: What's your choice?
Gynaecological cancers refer to the cancers that affect the female reproductive system such as the ovaries, uterus, cervix, fallopian tubes, vulva, and vagina. According to Eve Appeal, which is the U.K’s Gynaecological Cancer Research Charity, that raises awareness and funds research into the five common gynaecological cancers: Womb, Ovarian, Cervical, Vulval and Vaginal, there are over twenty two thousand new cases of gynaecological cancer every year in the U.K. Symptoms of gynaecological cancers may include pelvic and abdominal pain, bloating, abnormal vaginal bleeding, and changes in bowel habits. Early detection and treatment are crucial for the successful management of these cancers. Regular gynaecological screenings, including Pap tests and pelvic exams, can help detect these cancers in the early stages. Understanding the risks and symptoms associated with gynaecological cancers is important for all women to help prevent and manage these potentially life-threatening conditions.
Cervical screening, also known as a smear test, is an important preventative healthcare measure for women. The test involves taking a small sample of cells from the cervix to check for any abnormalities that could lead to cervical cancer. It is recommended that women aged between 25 and 64 years old should have a cervical screening every three to five years, depending on previous results, and those who are living with HIV should have one every year. Early detection of abnormal cells can lead to prompt treatment and a higher chance of successful outcomes. It is a simple and relatively quick procedure that can help to save lives, so it is important for all eligible women to participate in regular cervical screening.

Women in a park
There are two main types of cervical screening tests: the Pap test and the HPV test. The traditional Pap test involves collecting cells from the cervix and examining them under a microscope for any abnormal cells. This test can detect early signs of cervical cancer and is typically recommended for women aged 21 to 65. On the other hand, the HPV test checks for the presence of the human papillomavirus (HPV), which is the main cause of cervical cancer. This test can be done alone or in conjunction with a Pap test and is typically recommended for women aged 30 or older. It's important for women to discuss with their healthcare provider which type of screening is best for them and how often they should be screened.
Self swabbing tests have recently been introduced to allow women who would otherwise be uncomfortable with in-person tests or do not have time to attend in-person screening appointments. The self swabbing smear test is a much more convenient way to get checked for cervical cancer. Going for an in person smear test can be a daunting experience for some women. However, the self swabbing test can be done comfortably at home by following the instructions carefully. It also saves time and eliminates the need to visit a healthcare facility. On the other hand, an in person smear test is still necessary for some women, particularly those who may require additional medical attention or have difficulty performing the self swabbing test. Despite the slightly invasive nature of in person tests, they remain an essential part of women's health care, and they should never be ignored.
While i am all in favour of Self Swabbing for all the reasons listed above plus that it provides some sort of screening for those women who would have fallen through the cracks, i am still a firm believer in in-person smear tests because of the extra level of safety net it provides. Let me explain!

Woman sitting on couch
When i attend my smear test appointment ( which takes weeks of me psyching myself up), the nurse has a general conversation with me about how i am doing and if there have been any changes since my last smear test. Once i am lying down and in position and comfortable, she checks my vulva area for any changes, then feels for any swollen glands and once she is satisfied that everything looks healthy and alright, she inserts the speculum and continues with the smear test. Once all is done, i leave the appointment reassured that whilst i wait for my results, i am relaxed in the knowledge that my pelvic exam was otherwise normal and that i have no signs or symptoms of vulval cancer. But while in-person smear testing is my preferred choice of testing, i will leave you with the Pro and Cons of both, so that you can decide which one you would prefer, if not both.
Pros and Cons of Self-Swabbing Smear Test
Self-swabbing smear test is becoming more common as an alternative to the traditional method. There are pros and cons to consider when deciding whether to go for self-swabbing or not.
# Pros:
1. Less invasive - Self-swabbing test is less invasive because women do not require insertion of the speculum. This makes the procedure more comfortable for some women.
2. More privacy - Self-swabbing smear test allows women to perform the test in the privacy of their own homes. This enables women who find the traditional smear test embarrassing to have the test without feeling embarrassed.
3. Convenient - Women do not need to book an appointment or visit a clinic for a self-swabbing smear test. The self-swab can be done at home at a convenient time.
4. Cost-effective - Self-swabbing smear tests are usually cheaper than the traditional smear tests performed by medical professionals. This makes it a more affordable option for women who may not be able to afford the regular smear test fees.
# Cons:
1. Potential for inaccurate results - Self-swabbing may not be as accurate as the traditional smear test because the sample could be contaminated or insufficient,
Pros and Cons of In-person Smear Test
# Pros
Accuracy: In-person smear tests are generally more accurate than at-home tests.
Thoroughness: A healthcare professional can perform a more thorough exam during an in-person smear test.
Immediate Results: Depending on the facility, results can be available immediately after the test is performed.
Availability of Follow-up Care: If any abnormalities are detected, the healthcare professional can offer follow-up care or referrals for treatment.
Experienced Medical Professionals: The healthcare professional performing the test has undergone training and has experience in performing smear tests.
# Cons
Discomfort and Pain: For some individuals, smear tests can be uncomfortable or even painful.
Embarrassment or Shame: There may be cultural or personal barriers that make the test cumbersome or shameful to undergo.
Time and Effort: An in-person smear test requires scheduling an appointment and taking time out of one's day to travel to the facility.
So whichever method you choose, just remember that early detection saves lives and it is important to have your screening done when invited to have one.

The 5 Moments for Hand Hygiene.
Hand Hygiene practice is the simplest and most effective way of preventing infections.
The 5 moments for Hand Hygiene at the point of patient care, as adapted from the WHO Alliance for Patient Safety 2006 are:
1- Before patient contact
2- Before a clean/aseptic procedure
3- After body fluid exposure risk
4- After patient contact
5- After contact with patient surroundings
As a patient, you are well within your rights to question your Healthcare provider/ carer about hand hygiene.

Black and Menopause
Talking about being Black and Menopausal

Karen Authur on World Menopause Day
Today is World menopause day and we would like to bring you the brilliant work done by Karen Authur on raising issues around black menopause experience. She has a podcast where she talks all things black menopause with useful resources. You can follow her on her social media pages- Instagram: @menopausewhilstblack
And also link up to her linktr.ee:
https://linktr.ee/menopausewhilstblack
@thekarenarthur
----------------------------------------
Happy #WorldMenopauseDay
Image first posted two years ago. I was sick of not seeing diversity in the Menopause space. Plus I was tired of the same old 'Menopause is the end of life woe is me head in hands BS' tbh. Yes it can be shit. But that's often because we're not ready or prepared . We're not talking across generations. The medical profession are woefully under educated and society is constantly trying to silence older women. Don't get me started on what the world does to black women.
Anyway we're not having that any more are we loves?
We're two years on and much has changed culturally including new podcasts like mine @menopausewhilstblack with 2 seasons of honest knowledge centring the black British experience, new pod @blkmenobeyond and spaces like @mamm20_20 @blackwomeninmenopause and more.
Plus @davinamccall honesty in @muirka #SexMythsAndTheMenopause which blew viewing expectations out of the water, @themenocharity launched AND #CarolynHarrisMP will be speaking on dropping UK prescription charges for HRT (hormone replacement therapy) as well as mandatory menopause education for schools and colleges and workplace policies. There's a rally on the 29th October at 11.30am in Parliament Square, Londonium. If you can, come!
I'm thrilled to say that the UK seems to be leading the charge when it comes to discussion around menopause. But we still have a LOT to do.
This is an exciting time to be alive and kicking ass! I'm proud to be part of the generation to finally #MakeMenopauseMatter
Join us!
@dianedanzebrink Petition link is in my stories. Read more there. Then Sign it if you haven't and Share it with EVERYONE. Menopause is a GLOBAL, DIVERSE conversation!
I dun.
Peace xx
[Image description; Happy carefree older black woman laughs. White ombre text reads 'October 18th.World Menopause Day .Embrace the Change! "]
#MenopauseWhilstBlack
#MakeMenopauseDiverse
#BlackWomenInMenopause

Where do broken hearts go? A midnight reflection on mental health and mental health services within hospitals.

Patient in a hospital bed.
Everywhere you turn, you are reminded that we are living in unusual times, with words like “unprecedented” banded around often. We are also reminded of self care and mental well-being due to the effects of the pandemic and lock-down changing our way of lives for the foreseeable future if not forever- whats being called “the new normal”.
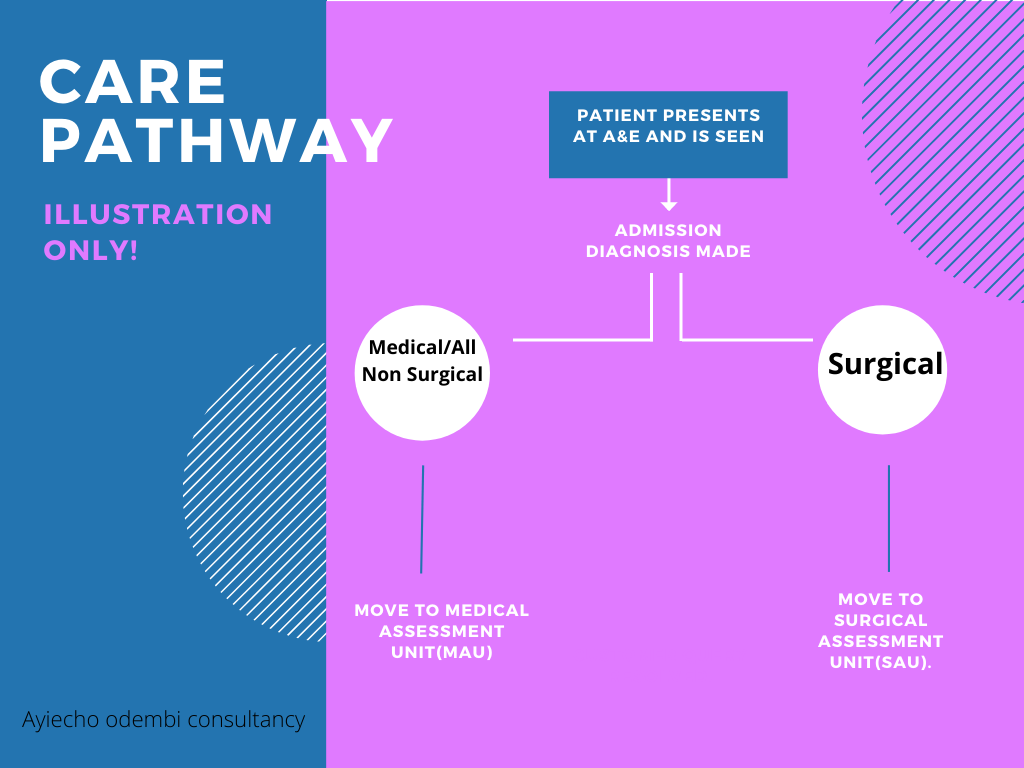
So there i was in the middle of the night, sleep having escaped me and Whitney Houston’s song ‘where do broken hearts go?’ playing over and over in my head, wondering where patients who presented with mental health problems went after coming into A&E? Or why , in my all my years in nursing, the only times i came across a mental health nurse was at university and when a psych consult was ordered on the unit/ward. Typically, when patients presented in A&E, and need admission, there are two routes normally followed- admission to the Medical assessment unit(MAU) or to the Surgical assessment unit(SAU). Most mental health patients end up in MAU or poisons unit( if admitted due to overdose and where such a unit is available and has empty beds).
Most of the time i have been involved in looking after a patient with mental health issues, it has been on an acute medical ward. This has been usually in the bays closest to the nurses patients reserved for patients who are acutely ill and need constant nursing supervision, which often involves bright lights, regular vital sign monitoring and other checks as per care plan with a hive of activity going on around due to the nature of varying acutely ill patients around. This got me wondering if an acute medical ward really is the right setting for someone going through a mental health crisis, given that they are being looked after by nurses, not mental health nurses, who yes might be doing a brilliant job and are good at what they do but are not aware of triggers or care pathways for someone going through a mental health crisis as a trained mental health nurse would with the patient in the right setting.

With a little help………
According to Mind¹, a leading mental health charity, mental health problems are common in England with 1 in 4 people experiencing some sort of mental health problem each year and 1 in 6 reporting having experienced a common mental health problem like anxiety or depression in any given week.
A study by The Nuffield Trust² looking at hospital use by people with mental health illness, makes for an interesting and sober reading and highlights a number of key points that need addressing. With almost every NHS hospital trust having a Medical assessment unit or a Surgical one, maybe it is time there was also a Mental health assessment unit where those coming into hospital with a mental health illness can get the care they deserve, looked after by trained mental health staff under conducive conditions designed with them in mind. I would certainly welcome a unit like that, where me and my fellow healthcare workers can pop into just for a chat or to make sense of life and all its challenges especially after a hard and emotionally draining day at work given the pressures we are constantly under with the added effect that this pandemic adds to it and i would be happy to know that mental health just like physical health, matters and that those going through any sort of mental health illness can come into hospital knowing that they have a dedicated area that’s ready to to help them in anyway possible.

Dr. Chisholm - the first Director-General of the World Health Organisation (WHO)

Focus on Informed Consent
Great Blog post below on the Patient Safety Learning site about Findings in the Cumberlege Review with a focus on Informed Consent. This is very relevant and important especially now that NHS Improvement England are looking into putting patients at the heart of patient safety.

Do Not Resuscitate- what do your family know?
14 years ago today my very patient better half almost killed me( it’s not what you are thinking).......well it could be argued that I was dead anyway but that's a story for another day ( when i almost became a Never Event statistic!).

A bag valve mask
14 years ago today my very patient better half almost killed me( it’s not what you are thinking).......well it could be argued that I was dead anyway but that's a story for another day ( when i almost became a Never Event statistic!).
It all started after an emotional episode of Greys’ anatomy where I declared I never want to be resuscitated but never got to really explain under what circumstances (I thought I had!). Well the day comes when I'm lying there being resuscitated x 3, himself in shock, resus successful, emergency surgery..... surgeon comes out to inform himself that they have managed to save me and that’s when he informs the surgeon that I'm against being resuscitated! We are all glad he failed to mention that while i was being resuscitated prior to surgery. I have now clarified the circumstances under which i would not want to resuscitated .
Have you talked to and explained to your loved ones your wishes when it comes to #resuscitation #endoflifecare

Nursing Standard on Instagram 16th March 2020
Nursing standard¹ have a great article about Marie Curie’s Talkabout campaign, that encourages people to openly talk about death and dying. They also had a feature on nursing and DNACPR orders², that clarifies the Nursing and Midwifery councils position on nurses who don’t start CPR where a DNACPR order is in place.
Links to the articles can be found below.
Nursing Standard( Linkedin): https://rcni.com/nursing-standard/opinion/comment/talking-about-death-and-dying-covid-19-has-taught-us-not-to-wait-161456 [Accessed June 2020]
Nursing Standard: https://rcni.com/nursing-standard/newsroom/news/nursing-and-midwifery-council-clarifies-its-position-nurses-who-do-not-start-cpr-159536 [Accessed June 2020]